Nashwa Khalid
Background:
Contact tracing aims to identify all potential transmission contacts from a source individual (known as an ‘index case’). This reveals a new set of individuals who might be infected and who can be the subject of further tracing effort. Traditionally, contact tracing for disease investigation are constructed only with personal contacts since personal contacts are the most identifiable paths for disease transmission. However, for Multi Drug Resistant TB (MDR-TB) where reducing time to diagnosis and consequently treatment is imperative in reducing the incidence, incorporating SNA into contact tracing may reveal potential contacts among patients and provide additional insights in MDR-TB transmission.
I plan to use survey data, to be collected by the TB Clinic at Indus Hospital (Karachi, Pakistan) to investigate the efficacy of employing SNA for contact tracing for MDR-TB patients, currently on treatment, in identifying new TB cases.
The Potential of SNA in Infectious Disease Control:
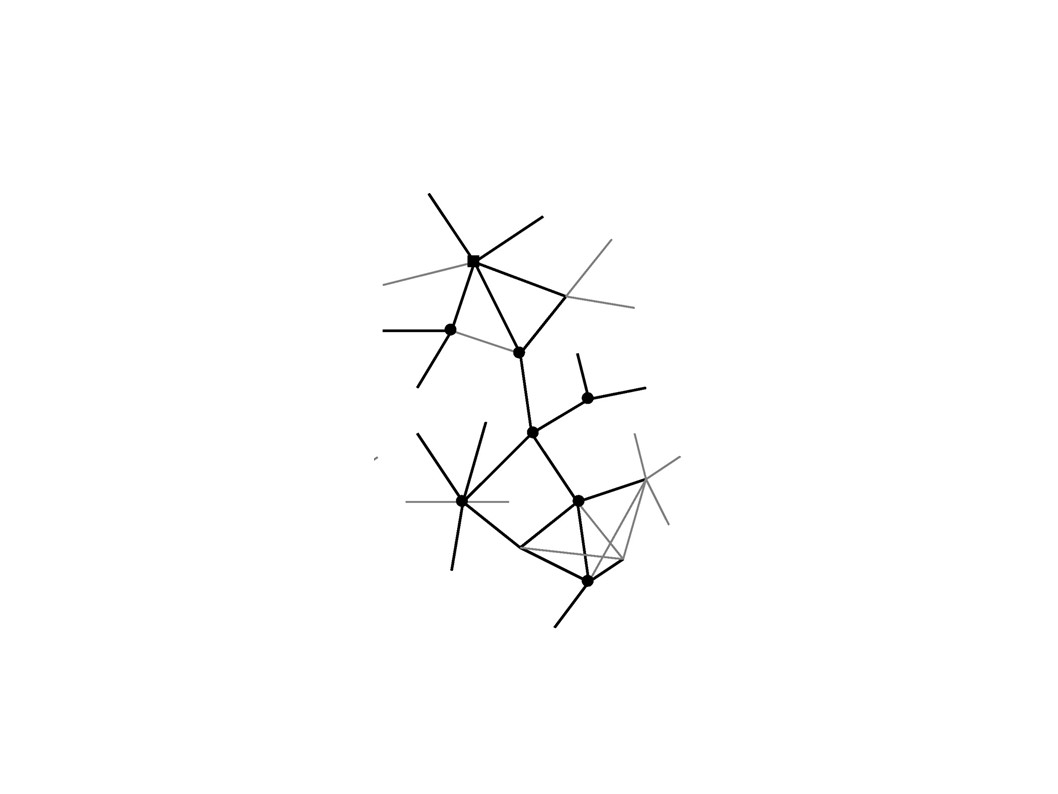
For a simple network
(thin grey lines), the type of network information that is achieved using SNA
incorporated contact tracing.
For contact tracing,
circles represent infected individuals, while the square shows the primary
infectious case. This method allows us to trace sources of
infection wherein a proportion of all contacts from
infectious individuals are traced.
Matt
J Keeling, and Ken T.D Eames J. R. Soc. Interface 2005;2:295-307
Hypothesis:
Research Questions:
1. Can the contact tracing network model visualized using Social Network software serve as a programmatic tool for public health programs in planning interventions for TB control.
2. Can contact tracing in conjunction with SNA be useful for epidemiological modelling to predict transmission patterns for similar populations in other cities in Sindh, Pakistan? This question is informed by the pioneering study of social networks carried out in Australia (Klovdahl et al. 1977)[1], where study participants were questioned about their social connections and by tracing some of these contacts a picture of a city-wide network of epidemic spreads was obtained.
Methods:
Surveying the individuals in the network to identify the relationships and map TB transmission or potential TB transmission.
· Use UCINET and NetDraw to visually map out the network.
· Review the map and the problems and opportunities highlighted using interviews and/or workshops.
· Designing and implementing actions to bring about desired changes.
· Mapping the network again after a suitable period of time
Important Network Measures
1. Centrality measures;
- Degree centrality– Which will help identify the number of people a patient has been exposed to and thus potential contact cases.
- Betweenness centrality – Which will give a measure of the proportion of times an infected individual lies on the path between other individuals
- Closeness centrality – As a measure of how long it will take to spread the infection from a node v to all other nodes sequentially.
2. Clusters: This can be used to identify characteristics of dyads, triads, and other subsets. For example, in an article about risk potential for HIV infection Friedman et al. used subgroup analysis to find all the components comprised of individuals in the network that had two or more drug-injecting or sexual links. They determined that this subset of individuals was an appropriate target for HIV prevention efforts because they were more likely to be HIV positive or engage in high-risk behaviors. A similar targeted approach can be employed by Indus Hospital for TB control.
I expect the focus of my analysis at the individual level to consist of identifying the position or location of actors in the network who play central roles, for example, those who are chosen more frequently by other network members (high eigenvector) or who act as brokers in communication or transmission networks (high betweenness). Additionally I expect three positions in social networks to be highly associated with transmission of health behaviors: isolate, bridge, and clique member.
As a side analysis; I would also like to tag any isolates, or patients with few or no links to others, for further inspection. I hypothesize that isolates, due to a lack of support structure and given the length/difficulty of TB treatment regimen will be more likely to default on treatment. As defaulting on TB treatment increases the risk of developing Extensively Drug Resistant TB (XDR-TB) these individuals can be targeted by Indus Hospital for additional counseling and home visits.
Current Literature and Similar studies:
Study Design:
My sampling method will be snowball sampling; wherein we will have to interview an infected patient so find a tie to another actor of interest (person with suspected TB or another diagnosed TB patient), interview them and repeat the process until the desired sample size is reached.
The study must define how much contact is it necessary to have with someone with TB, before there is a measurable risk. Different types of relationship bestow different risks and judgments must be made about which sorts of transmission routes are likely to be significant in TB transmission. One way around this problem is to employ valued networks in which links are not merely present or absent but are weighted according to their strength; which for the purpose of the study will be:
- Frequency of contact between individuals eg. On a scale of 1 – 3, where 3 - Frequent, 2- Often, 1 - Sometimes
1. Occupation and place of employment.
2. Number of employees at place of employment
3. Where do you spend most of your time, aside from your residence?
4. Common mode of transport
5. Have you traveled outside Karachi since being diagnosed or in the past three months (whichever is the most recent option)?
6. Please list ten people you spend the most time with on average (coded for relationship to patient eg. 1- Family member, 2- Friend, 3- Colleague, 4-Acquaintance)
7. Please list all the people you know who have been diagnosed with TB (coded for relationship to patient eg. 1- Family member, 2- Friend, 3- Colleague, 4-Acquaintance)
[1] Klovdahl A.S,
Dhofier Z, Oddy G, O'Hara J, Stoutjesdijk S, Whish A 1977 Social networks in an
urban area: first Canberra study Aust. N. Z. J. Sociol. 13, 169–172
[2]Kretzschmar, M. and M.
Morris 1995 "Measures of concurrency in sexual networks and the spread of
STD." Mathematical Biosciences, in press.
[3]Klovdahl, A.S. 1985
"Social networks and the spread of infectious diseases. The AIDS
example." Social Science and Medicine 21: 1203-1216
[4]Watts, C.H. and R.M. May
1992 "The influence of concurrent partnerships on the dynamics of
HIV/AIDS." Mathematical Biosciences 108: 89-104
[5]Lisa K. Fitzpatrick, Jo
Ann Hardacker, Wendy Heirendt, Tracy Agerton, Amy Streicher, Heather Melnyk,
Renee Ridzon, Sarah Valway, and Ida Onorato
A Preventable Outbreak
of Tuberculosis Investigated through an Intricate Social Network
2 comments:
If you were doing an actual study, you'd want your hypothesis to me more specific, and something that you could prove or disprove using social network analysis. Just hypothesizing that it is useful isn't enough. Your second sub-question is interesting though, and would be a great basis for a study.
-Miranda
I agree with Miranda's comment about the Q, and I appreciate the amount of research you did on the topic. Hope you'll get to follow through on this someday.
Post a Comment